The COVID-19 pandemic is one of the major challenges of our time. Many of us would advocate for evidence-based policy: we should let science guide us on the best course of action. Unfortunately, a complete lack of evidence for our current approach means the way forward is unclear.
The evidence for the lockdown
At first glance, it seems self-evident that implementing a lockdown will reduce deaths. If we all stay at home, it will reduce the transmission of the disease. In theory, this should allow us to spread the disease out over a longer period, and thus avoiding the healthcare system becoming overwhelmed.
Unfortunately, the evidence does not support this view. A Cochrane Review from 2011 concluded “there was limited evidence that social distancing was effective, especially if related to the risk of exposure.”
At the moment, we don’t even understand how dangerous COVID-19 is. As Dr John Lee notes in his article in The Specator, the lack of testing means the mortality stats are meaningless. We’re comparing deaths to confirmed cases, but the untested cases are anywhere from three times as many to three hundred times as many if a recent study by Oxford University is to be believed.
This is confounded by COVID-19 being a “notifiable disease”, meaning that a death could be reported as COVID-19 when a patient actually died of something else. This seems highly plausible given the average age of COVID-19 deaths is 79.5.
As Professor John Ioannidis points out, due to the lack of evidence, the policies we implement could hinder rather than help.
School closures, for example, may reduce transmission rates. But they may also backfire if children socialize anyhow, if school closure leads children to spend more time with susceptible elderly family members, if children at home disrupt their parents ability to work, and more. School closures may also diminish the chances of developing herd immunity in an age group that is spared serious disease.
Even if we somehow did concede there was some evidence for social distancing, we do not need to confound this idea with a lockdown. You can implement social distancing: such as getting people to work from home and banning large gatherings, without implementing a lockdown in which nobody is allowed to leave their house.
Further, even if social distancing did turn out to reduce infection rates overall, we need to look specifically at how it affects the elderly and vulnerable. It could be that young healthy professionals can lock themselves away and avoid infection, but those who require carers coming in and out of their home, or those who need regular medical appointments, cannot. Another example of how social distancing can harm, rather than hinder because the natural immunity we would otherwise develop from the age-groups at the least risk is never built up.
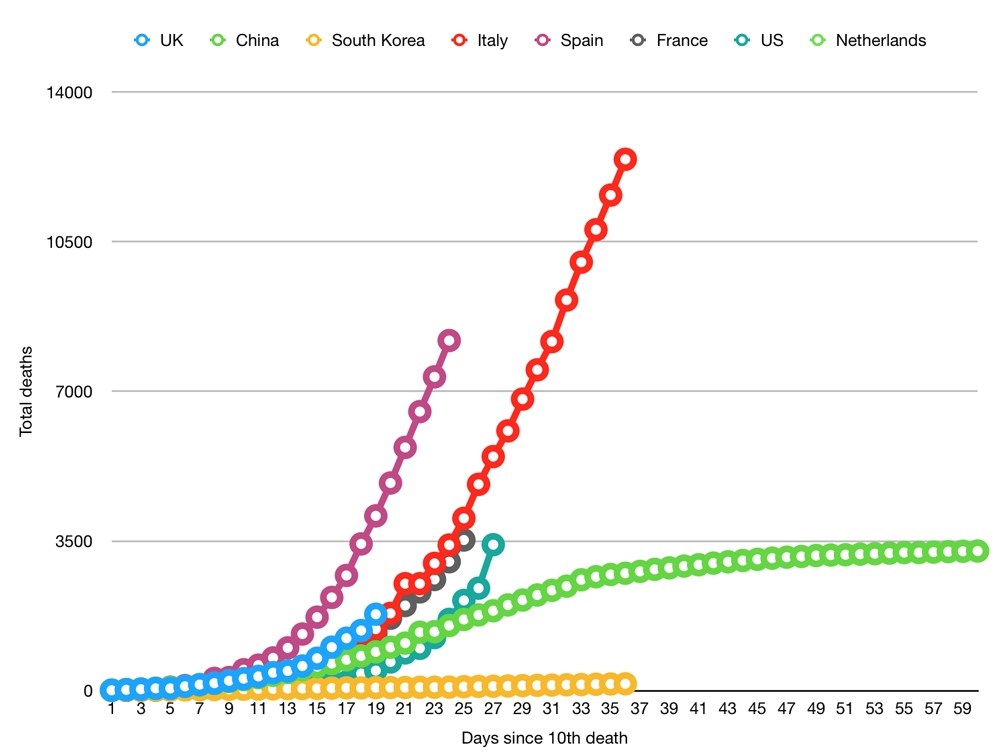
Ultimately, then, the evidence for social distancing is not substantiated. It could be that the models from Imperial College London are correct. But they may also be utterly incorrect. And that is serious as I will explain below.
Social costs of a lockdown
A lockdown is a serious thing in itself. It violates both Article 3 and Article 13 of the UN Declaration of Human Rights. If you are a Brexit-voter who supported leave because you were tired of human rights, you might like the sound of that. But most of my friends are fellow lefties who quite like human rights.
You could argue that is worth it temporarily to protect public health. And maybe it is. But we need to take all of the consequences into account.
These vary from the (arguably) mild: people have had their lives put on hold. They are not allowed to do the things they enjoy, like seeing the people we love. And doing the things we love: whether that is music festivals, triathlons, pub quiz nights or basically any hobby that doesn’t involve sitting on your sofa.
And continue up to the very serious:
- Children are being stripped of their education. It’s impossible to expect parents to homeschool to the standard of professional teachers, and so much of education is the social education of interacting with peers and the school system.
- Some children only get hot meals in school.
- University students who are paying £9,000 per year tuition fees are not receiving their education
- The cost to people’s mental health of being socially isolated and not going outside as much.
- The resulting increase of suicides.
- The transfer of healthcare resources from other conditions to COVID-19. Doctors and dentists are no longer offering appointments and operations for non-life-threatening but nevertheless debilitating conditions have been cancelled
- The tidal wave of anxiety from people wondering whether they have a job tomorrow, or already having lost their job
- The self-employed who find their income has suddenly disappeared and that they are not eligible for government support (which covers nowhere near 95% of self-employed people as the Chancellor claimed)
- The already-overstretched police services admitting that they will only be investigating the most serious crimes because they will be too busy enforcing the lockdown
- The domestic abuse victims who we have locked in a building with their abuser, and given their furloughed abuser nothing better to do than sit around and drink.
- Drug and alcohol users who are in recovery but now more likely to relapse.
These are really, really bad.
People who have flouted the social distancing rules have rightly been called callous towards more vulnerable members of society. But we need to be careful not to fall into the same trap. To dismiss the social costs because our mental health is not suffering, because we have not lost our job, or because we don’t have children who spend years working exams they are now not allowed to take, nor even say goodbye to their lifelong school friends, is a privilege many other people in society do not enjoy.
As Lee puts it, “the moral debate is not lives vs money. It is lives vs lives. It will take months, perhaps years, if ever, before we can assess the wider implications of what we are doing.”
Weighing up the costs
Some young people have died from COVID-19 and that quite rightly tugs the heartstrings. But emotion is very different from evidence. And the evidence from Oxford University shows that the average age of those dying is 79.5.
Life expectancy in the UK is 81. That’s a loss of a year and a half, which is a serious and significant difference. I would be heartbroken if I lost my grandmother 18 months prematurely.
But we have to weigh that against the real and serious damage we are doing to everyone in society. Imperial’s modelling, which has formed much of the basis of the current strategy, predicts that social distancing and lockdowns will have to continue intermittently but indefinitely while we wait for a vaccine. Said vaccine will take at least 18 months to develop, even if everything goes smoothly, and that is before we even start the even bigger hurdle of global immunisation.
If we truly are looking at a 2+ year timescale, the cure would seem worse than the disease. With the average life expectancy of a COVID-19 victim only being 18 months, the majority are likely to die of natural causes in the meantime, doomed to be cremated at a funeral that nobody is allowed to attend.
Worse still, it may be that, as many commentators have predicted, social distancing and lockdowns are not sustainable for such a long period of time. As a result, the pandemic will continue to flare up and kill just as many people, and all our suffering will have been in vain.
If the pandemic magically goes away in the next 12 weeks, then you can make a solid case for the lockdown. And let’s pray that it will. But if not, and we have to keep the suppression methods in place until the vaccine arrives, or they simply fail, we will have wasted more of everyone’s lives than we saved for the 0.25-1% of people who, already at the end of their life, had it cut slightly shorter.
Ultimately, we do not know what the correct answer is. A lack of testing and a lack of data means the conclusion is unclear. And yet, based on that, we are implementing a policy with dire consequences for education, mental health and quality of life.
Editing notes: reflecting back, I’m not sure 81 is a fair assessment of life expectancy. Although it is the average life expectancy in the UK, once you reach 79.5, you are likely to live longer than 81. How we adjust for this is unclear, though. The ONS suggests that a 79-year-old will live another eight years. But this is for a typical person, and we know that most people survive the virus but that rates of mortality are particularly high for people with underlying health conditions. Therefore, in order to adjust, we would need to know the life expectancy of a 79-year-old with underlying health conditions. Unfortunately, that is data we do not have.